By
Dr. Deepak Gupta  ,
Dr. Arvind Srirajakalidindi
,
Dr. Arvind Srirajakalidindi 
Corresponding Author Dr. Deepak Gupta
Wayne State University, - United States of America 48201
Submitting Author Dr. Deepak Gupta
Other Authors
Dr. Arvind Srirajakalidindi
Detroit Medical Center, Anesthesiology, - United States of America
Jaw-Thrust, 2-Rescuers, Hands-Only CPR
Gupta D, Srirajakalidindi A. Add Jaw-Thrust To Evolve 2-Rescuers Hands-Only CPR. WebmedCentral CARDIOLOGY 2019;10(9):WMC005593
This is an open-access article distributed under the terms of the Creative Commons Attribution License(CC-BY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
No
My opinion
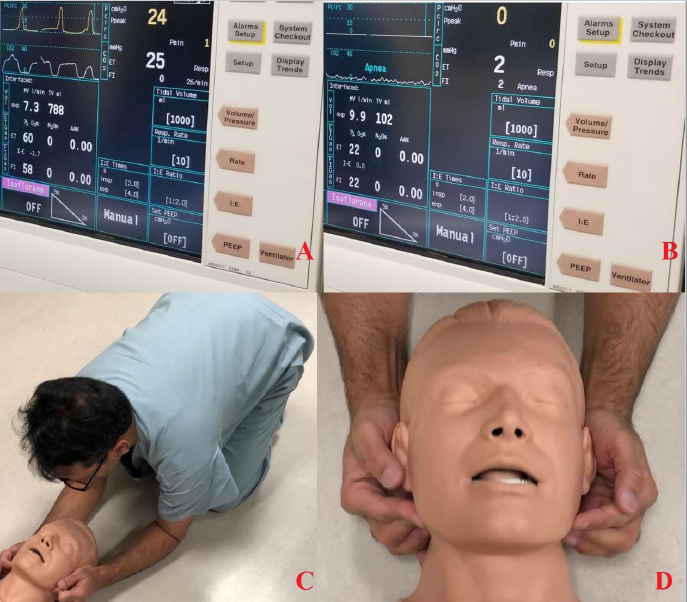
Cardiocerebral resuscitation (CCR) as an evolved form of cardiopulmonary resuscitation (CPR) has been termed as Hands-Only CPR (HOCPR) for the lay rescuers.[1] iStan Adult Patient Simulator (CAE Healthcare, Saint-Laurent, Quebec, Canada) provides definitive evidence of “covert” pulmonary resuscitation happening during CCR. During a simulated clinical experience (SCE), end-tidal carbon dioxide (ETCO2) obtained at baseline was 25 mmHg (Figure 1A) when providing 788 ml tidal volume (TV) breaths during manual ventilation of intubated iStan. Subsequently obtained ETCO2 was 2 mmHg (Figure 1B) when HOCPR generated 102 ml TV “breaths” in non-ventilated iStan with endotracheal tube open-to-room-air. Although delivery of prematurely early breaths during manual ventilation miscalculated respiratory rate (Figure 1A), minute ventilation (MV) equated to ~10 breaths/min during 7.3 l/min manual ventilation paradoxically increased to 9.9 l/min when ~100 compressions/min HOCPR generated 102 ml TV “breaths” (HOCPR-induced-high-frequency-“ventilation”). Essentially, the SCE with intubated iStan is making the case for keeping airway-and-mouth open during HOCPR. Therefore, HOCPR training should devise SCE for 2-rescuers HOCPR wherein second lay rescuers are providing jaw thrust with their elbows resting on the floor (Figure 1C-1D) to comfortably sustain jaw thrust and keeping airway-and-mouth open for prolonged periods during HOCPR. Moreover, future investigators should document if they observe that, after the end of each exhalation, there is evidence of measurable ETCO2 as “cardiogenic oscillations” during each inspiratory downstroke in intubated and manually or mechanically ventilated patients during the times when they are receiving continuous chest compressions. Thereafter, they should explore whether controlling wind-speed around the open mouth can improve the “inhalability” of breathing zone room air in apneic mannequins.[2-3] Summarily, even though the above-mentioned observed evidence of pulmonary resuscitation during CCR (HOCPR) may need further exploration and validation studies, adding jaw thrust in the interim to evolve 2-rescuers HOCPR may only contribute to bettering the process of CPR.
References
- Ewy GA: Cardiocerebral and cardiopulmonary resuscitation - 2017 update. Acute Med Surg 2017; 4:227-34
- Schmees DK, Wu YH, Vincent JH: Visualization of the airflow around a life-sized, heated, breathing mannequin at ultralow windspeeds. Ann Occup Hyg 2008; 52:351-60
- Anthony TR, Anderson KR: Computational fluid dynamics investigation of human aspiration in low-velocity air: orientation effects on mouth-breathing simulations. Ann Occup Hyg 2013; 57:740-57
Figure Legend
Figure 1: Evidence of Exhaled Carbon Dioxide (ETCO2) During HOCPR Prompting To Keep Airway And Mouth Open With Jaw Thrust During HOCPR [(1A): Baseline ETCO2 at ~25 mmHg During Manual Ventilation; (1B): Evident ETCO2 at ~2 mmHg During HOCPR; (1C): Schematically, Second Lay Rescuer Providing Jaw Thrust With Elbows Resting On Floor; (1D): Schematic Close Up View Demonstrating Jaw Thrust Providing Fingers’ Alignment]
Source(s) of Funding
NOT APPLICABLE
Competing Interests
NOT APPLICABLE
 All site content, except where otherwise noted, is licensed under a
Creative Commons Attribution License
All site content, except where otherwise noted, is licensed under a
Creative Commons Attribution License